

Executive Summary
Introduction
Milton Keynes City is focused on tackling local health inequalities that start before birth and accumulate throughout life. It understands that these inequalities are preventable and to achieve the best outcomes it is necessary to focus on the complex influences affecting children and young people’s health, including their family, environment, life skills, knowledge and experience. Preventing or minimising the impact of risk factors, including adverse childhood experiences, is vital. It is equally important to strengthen the protective factors, particularly the resilience (ability to cope) of your children, young people, and their families.
Role of deprivation
Deprivation, which is measured by a combination of income, employment, education, health, housing and services, living environment and crime factors, is recognised as a major contributing factor in inequalities to health outcomes. Indeed, a report by the National Children’s Bureau into health inequalities in England found that children and young people growing up in more deprived areas tend to have worse health outcomes, but also found that this was not inevitable.1
The health and wellbeing of children and young people in Milton Keynes City are generally better than the England average. However, as is seen generally across the country, there is significant variation in outcomes within the area; some groups of children and young people have significantly worse health outcomes than others. In particular, deprivation varies considerably across the area and more on how deprivation is calculated for Milton Keynes can be found here.
Activities and actions
The Healthy Child Programme (HCP) offers a range of interventions for all children, young people and their families in Milton Keynes City from pre-birth to 19 years.2 There may be times in childhood and adolescence when additional help and support is needed. Earlier identification enables a timely and effective response before issues escalate. The case for early help and intervention is well evidenced, as is the need for a skilled, multi-agency workforce that communicates well and works together. No single agency can provide support on its own.3
Impact of Covid-19 pandemic
The pandemic caused unprecedented challenges for the health and wellbeing of children and young people – schools were partially closed and remote learning implemented, many non-essential services were closed, and social distancing strategies meant alternative ways of delivering health care were necessary. In addition, although many of social changes were universal there has been a disproportionate impact on children and families, exacerbating pre-existing inequalities.
1. Healthy Pregnancy
The circumstances and behaviours of parents and the wider family before the baby is conceived, during pregnancy, and once the baby is born, can either have a positive or negative effect on their child. Babies born to parents with disadvantageous circumstances and unhealthy behaviours have an increased risk of low birth weight, early illness and even early death. Intervening early will have an impact on a child’s resilience and their physical, mental and socioeconomic outcomes in later life.
Key findings
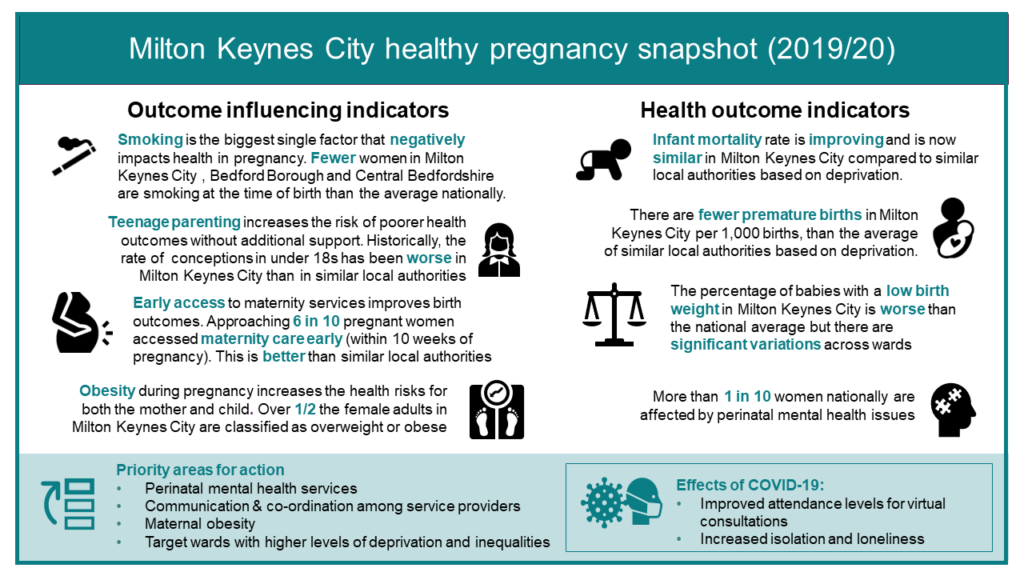
- The infant mortality rate in Milton Keynes has improved significantly. It is now 4.4 per 1,000, which is similar to local authorities in the same deprivation decile.
- Milton Keynes performs significantly better than similar local authorities for women accessing maternity care within 10 completed weeks of pregnancy (57.6%).
- Although the percentage of women known to be smokers at the time of delivery has reduced, this remains high at 12% of all maternities.
- The under 18 conception rate has decreased compared to the previous year.
Impact of COVID-19
- During the first wave of COVID-19, face-to-face consultations were replaced with virtual consultations, as were antenatal educational classes. Greater attendance by parents were noted for these.
- However, there has been an increase in loneliness and isolation, and increased maternal anxiety associated with these changes.
Priority actions to deliver better outcomes:
- Roll-out ‘Continuity of Carer’ for all women, to address many of the pre-existing health inequalities – and reduce the likelihood of mums having preterm births, losing their baby in pregnancy or in the first month following birth.
- All Milton Keynes services throughout the maternity journey should listen to women and their partners, ensure their voices are heard, and respect their informed choices, by personalising their care.
- Improve information sharing systems between maternity and health visiting services to ensure prompt access to the full Healthy Child Programme.
- Develop and co-produce maternal mental health services associated with grief, loss and trauma to meet the current gap in provision.
- Review the effectiveness and impact of the parental mental health pathway – with a particular focus on ethnic minority families – to address mental illness during the perinatal period.
- Ensure services for parents and carers are personalised and are able to provide choices for how they access support, including both face to face and virtual provision.
- Develop and monitor a training programme to improve skills of service providers to provide a more effective tailored approach to supporting women with reducing tobacco dependence.
- Ensure effective measurement and recording of BMI, and referral to appropriate weight management services, both antenatal and postnatal as identified in the Maternal Obesity Pathway.
2. Health Birth and Early Years
Families are the most important influence on a child during these years, and early identification of families who need help combined with evidence-based interventions is key to improving outcomes. We are aiming for parents and carers to feel supported to make decisions to improve their child’s health outcomes and life chances, be their child’s first educator, and feel confident to manage their child’s minor illnesses and health issues.
Key findings
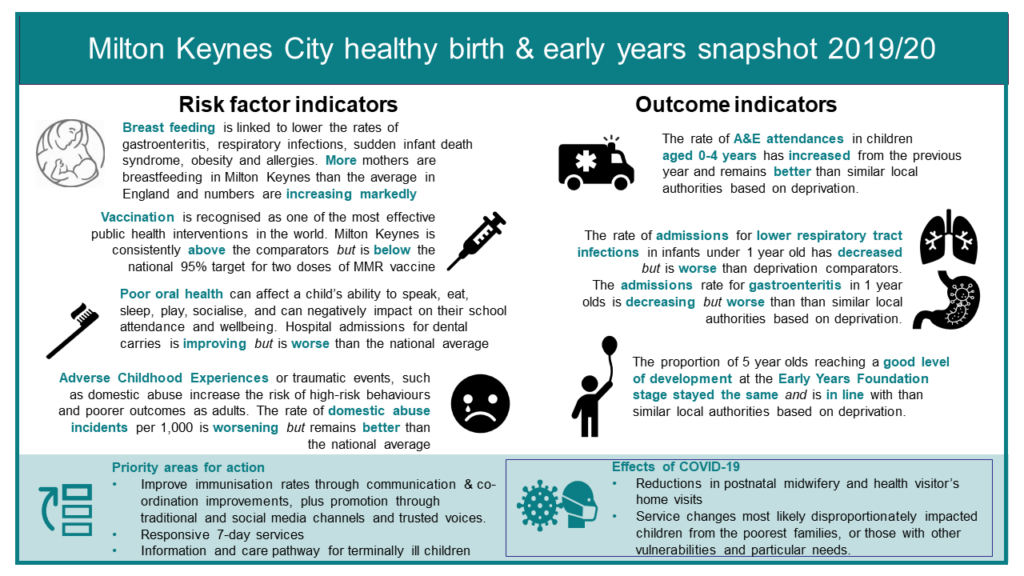
- Breastfeeding is an important protective factor – in Milton Keynes 80.4% of women initiate breastfeeding, which is a marked increase from 58.5% the previous year and higher than the England average (74.5%). Unfortunately, data is not available locally regarding breastfeeding at 6-8 weeks.
- 8.5% of all babies are born at a low birth weight (under 2500g). This remains significantly higher than local authorities of similar deprivation.
- Milton Keynes performs significantly better than similar local authorities for the rate of A&E attendances in children aged 0-4 years – 373.3 per 1,000 compared to 590.3 per 1,000.
- However admissions in children under 1 year old for both gastroenteritis and lower respiratory tract infections are significantly higher in Milton Keynes than local authorities of similar deprivation (125. per 1,000 and 981 per 1,000 respectively).
Impact of COVID-19
- During the pandemic, although partners have been able to support women during their birth, visits to labour, antenatal and postnatal wards were reduced. There has been a reduction in postnatal midwifery and health visitor’s home visits.
- Although postnatal visits were changed to telephone or virtual consultations, more mothers were breastfeeding at 6-8 weeks. The reasons for this are unclear.
- During the COVID-19 pandemic, in Milton Keynes there has been partial closure of some nurseries, and group activities in Children’s Centres being suspended.
- Changes during this time are likely to disproportionately impact children from the poorest families, or those with other vulnerabilities and particular needs.
Priority actions to deliver better outcomes:
- The ICS/Public Health/NHSE and all key stakeholders in delivering vaccination to children and young people to work together to continually raise the profile of immunisation, monitor activity and identify and address issues such as increased vaccine hesitancy in certain communities, in a timely manner.
- Support with effective positive messages around immunisations to parents and young people.
- Using the most appropriate and effective means to communicate messages, for instance, social media and trusted voices.
- Support with access to appropriate community vaccination venues to provide easy access for all children who have not been vaccinated in a school setting.
- Population awareness of choice of vaccine for the healthy children’s flu programme to include non-porcine vaccine.
- Responsive 7-day services to cater to the needs of children and young people and carers to ensure children get care close to home at the right place at the right time.
- Continue to ensure a focus on identifying and addressing modifiable factors arising during reviews.
- Continue to ensure information about any child deaths reviewed that meet the criteria for a Learning Disability Mortality Review (LeDeR) are reported to and shared with LeDeR.
- Monitor the palliative care pathway and promote support to bereaved families.
- Embed the use of the eCDOP system across the Milton Keynes workforce
3. The School-Aged Years
The Chief Medical Officer and Professor Sir Michael Marmot have highlighted the importance of giving every child the best start and reducing health inequalities throughout life. They recognise the importance of building on the support in the early years, and sustaining this across the life course for school-aged children and young people to improve outcomes and reduce inequalities through universal provision and targeted support.
There will be challenges within a child’s or a young person’s life and times when they need additional support. Universal and targeted public health services provided by health visiting and school nursing teams are crucial to improving the health and wellbeing of all children and young people.
Key findings
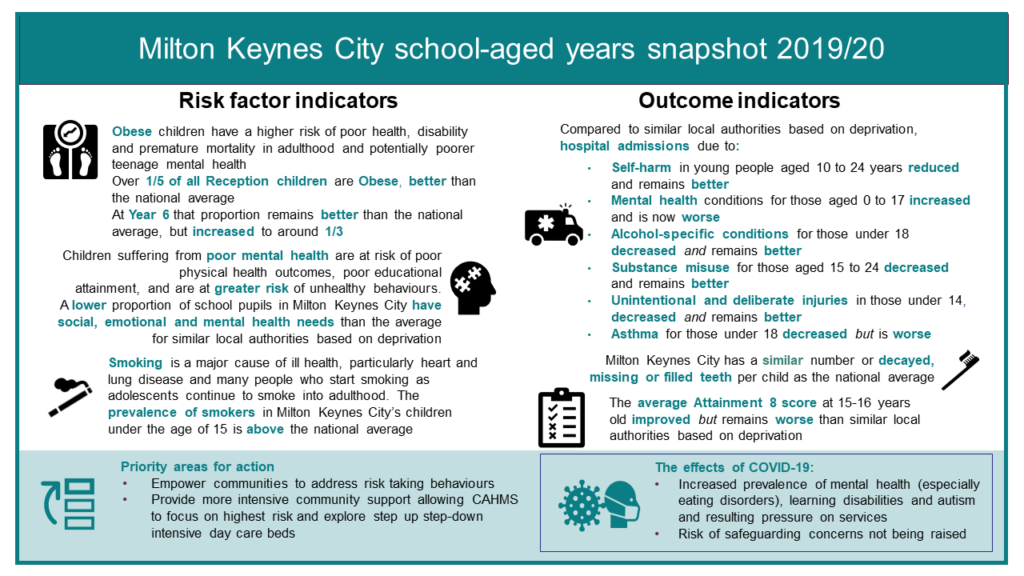
- 21.2% of children in Year R, and 33.2% of children in Year 6 are overweight or obese. This is significantly better than the England averages.
- Performance for Attainment 8 is significantly lower than similar local authorities – a mean score of 48.8 compared to 51.6
- 2.22% of school pupils have social, emotional or mental health needs, which is low compared to similar local authorities
- • 5.7% of 16-17 year olds are not in education, employment or training (NEET) – significantly higher than 4.2% for the deprivation decile
- Milton Keynes performs significantly better compared to local authorities of similar deprivation regarding hospital admissions for a range of conditions:
- alcohol-specific conditions in under 18s
- admissions caused by unintentional and deliberate injuries in children aged 0-14 years
- hospital admissions as a result of self-harm in children aged 10-24 years
Impact of COVID-19
- Schools in England closed at the beginning of the pandemic, with remote learning being rolled out to support children and young people to continue learning at home (with the exception of vulnerable pupils and children of key workers). National exams were cancelled for 2020 and 2021.
- We have seen both increasing numbers and increasing acuity of children and young people suffering crisis, whether it is due to mental ill health, or related to learning difficulties and /or autism. There has been an unprecedented surge in presentations for eating disorders.
- The increase in children and young people with mental health difficulties has greatly increased the pressure on GPs, Child and Adolescent Mental Health Service (CAMHS) Tier 4 beds, hospital paediatric beds, and crisis teams. It has also presented additional challenges for schools.
- Reductions in face-to-face meetings and contact with professionals has led to fewer safeguarding concerns being raised. Schools and colleges are the highest referees into safeguarding systems, and children and young people have not been physically in education settings during this time. Child exploitation may potentially increase, in particular online exploitation due to increased regular use of technology.
- Professionals are very mindful of the impact the pandemic may have on safeguarding concerns, and are building capacity to take account of the projected increase in demand on services as systems begin to return to normal.
Priority actions to deliver better outcomes:
- Encourage coproduction with young people (and their families and schools) across Milton Keynes in order to explore issues related to health and wellbeing and the impact that COVID on access to services and support.
- Ensure services for young people are personalised and are able to provide choices for how they access support, including both face to face and virtual provision.
- Adapt the CAMHS models to focus on higher risk young people and to provide more intensive community support.
- Rapidly explore the potential for step up and step down beds/ intensive day care (potential solution for the increased number of CYP needing intensive support for eating disorders) Inpatient provision and local bed management
References
- National Children’s Bureau. 2015. Poor Beginnings: Health Inequalities among Young Children Across England. [online] Available at:
http://www.ncb.org.uk/sites/default/files/uploads/files/Poor%2520Beginnings.pdf [Accessed 16 December 2020] - Public Health England. 2020. Rapid Review to Update Evidence for the Healthy Child Programme 0–5. Available at:
http://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/429740/150520RapidReviewHealthyChildProg_UPDATE_poisons_final.pdf [Accessed 16 December 2020]. - Public Health England. 2019. Healthy Beginnings: Applying All Our Health. Available at:
https://www.gov.uk/government/publications/healthybeginnings-applying-all-our-health/healthy-beginnings-applying-all-our-health [Accessed 16 December 2020].